Therapeutic ERCP: A Lifesaving Procedure for Biliary Obstruction from Gallstones and Cancer
Introduction
Biliary obstruction is a serious condition that occurs when the flow of bile from the liver to the small intestine is blocked. This blockage can result in jaundice, severe infection, liver damage, and even life-threatening complications if not addressed swiftly. One of the most effective treatments for this condition is therapeutic ERCP (Endoscopic Retrograde Cholangiopancreatography).
Therapeutic ERCP is a specialized endoscopic procedure that allows gastroenterologists to diagnose and treat issues in the bile ducts, pancreatic ducts, and gallbladder. It is especially beneficial for patients experiencing biliary obstruction due to gallstones, strictures, or cancer.
In this article, we will discuss what therapeutic ERCP is, its indications, what patients can expect during the procedure, and the importance of timely intervention.
Understanding Biliary Obstruction
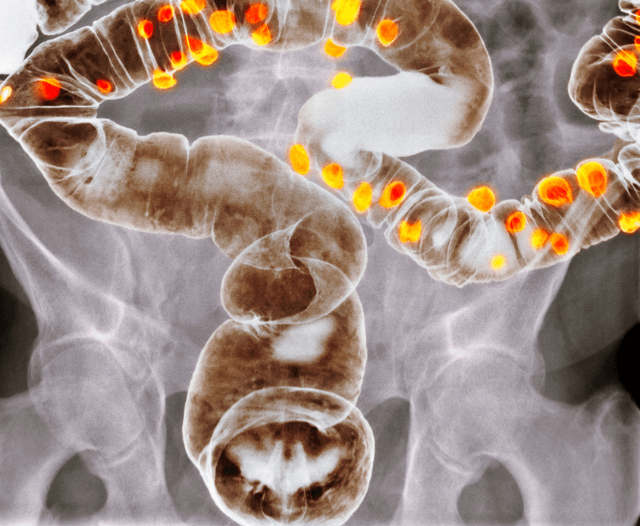
The biliary system consists of a network of ducts that transport bile—a fluid produced by the liver—to the small intestine to aid in fat digestion. A blockage in these ducts causes bile to back up into the liver and bloodstream.
- Gallstones in the bile duct (choledocholithiasis): Stones may migrate from the gallbladder into the bile duct, causing pain, infection, and jaundice.
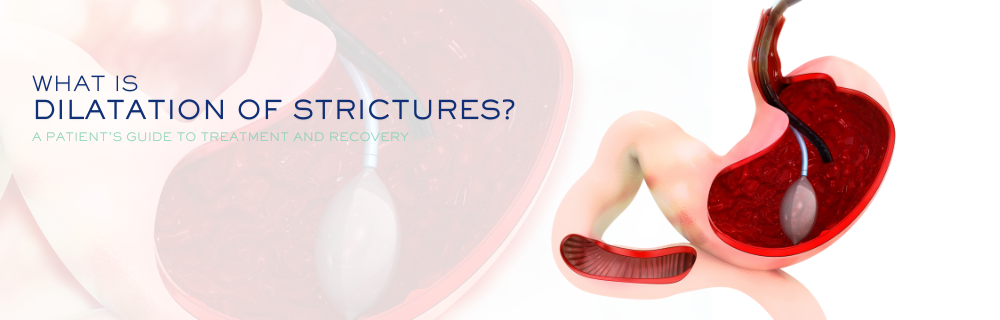
- Biliary strictures: These are narrowings of the bile ducts, which can result from scarring, inflammation, or surgical injury.
- Cancer: Tumors in the bile duct, pancreas, or gallbladder may compress or invade the bile ducts.
- Other causes: Rarely, parasites, chronic pancreatitis, or congenital abnormalities can also lead to obstruction.
Symptoms of biliary obstruction include:
- Yellowing of the skin and eyes (jaundice)
- Dark urine and pale stools
- Severe upper abdominal pain
- Fever and chills (which may indicate infection)
- Nausea and vomiting
- General fatigue and itching
If untreated, biliary obstruction can progress to cholangitis (a severe infection of the bile ducts), sepsis, liver failure, and other complications. Prompt diagnosis and treatment are, therefore, essential.

What Is Therapeutic ERCP?
ERCP is a minimally invasive procedure that combines endoscopy with fluoroscopy (X-ray imaging) to diagnose and treat biliary and pancreatic disorders.
While diagnostic ERCP is used mainly to visualize the bile and pancreatic ducts and identify blockages, stones, or tumors, therapeutic ERCP allows for the treatment of these issues in the same session.
Through therapeutic ERCP, gastroenterologists can:
- Remove gallstones from the bile duct
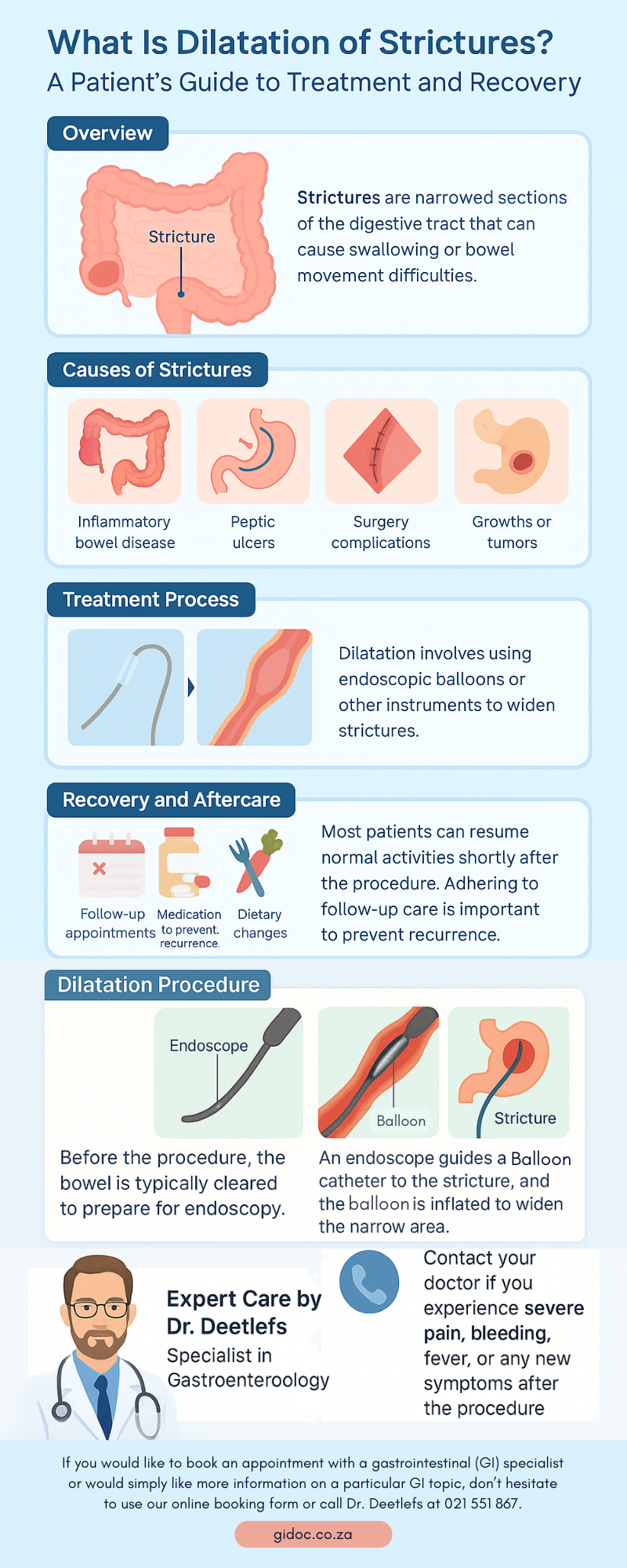
- Widen narrowed ducts (stricture dilatation)
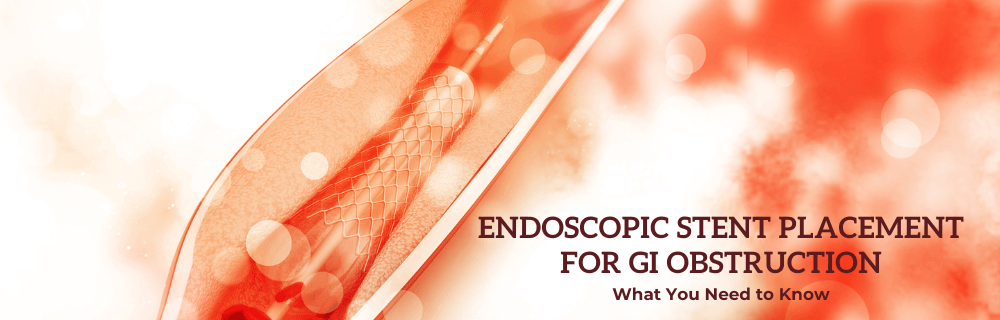
- Insert stents to relieve obstructions caused by cancer or scar tissue
- Perform a sphincterotomy (cutting the muscle at the duct opening) to improve bile flow
- Drain infected bile, which is particularly important in managing cholangitis
This dual diagnostic and therapeutic capacity makes ERCP a crucial tool in modern gastroenterology.
How the Procedure Works
- Preparation:
- Patients are typically required to fast for several hours before the procedure. Blood tests may be conducted to assess liver function and clotting abilities.
- Sedation:
- ERCP is generally performed under conscious sedation or general anesthesia, depending on the patient’s needs and the complexity of the procedure.
- Endoscopic Access:
- The gastroenterologist advances a flexible endoscope through the mouth, esophagus, and stomach into the duodenum (the first part of the small intestine).
- Cannulation and Contrast Injection:
- Using specialized instruments, the physician locates the opening of the bile duct (papilla), inserts a catheter, and injects contrast dye to visualize the ducts under X-ray.
- Therapeutic Intervention:
- Stone Removal: A balloon or basket device is used to extract stones.
- Stent Placement: Plastic or metal stents are inserted to keep the ducts open when narrowed by cancer or scarring.
- Sphincterotomy: A small incision is made to enlarge the bile duct opening, improving drainage.
- Post-Procedure Care:
- Patients are monitored during recovery for several hours. Most can return home the same day unless observation is required due to infection or complications.
Benefits of Therapeutic ERCP
- Immediate Relief of Symptoms: Rapidly removes obstructions, reducing jaundice, pain, and infection risk.
- Minimally Invasive: Requires no large incisions, promoting faster recovery compared to open surgery.
- Combined Diagnosis and Treatment: Allows for both in a single procedure, minimizing delays.
- Essential for Cancer Care: Stenting in malignant obstructions relieves jaundice and enables timely chemotherapy or surgery.
Risks and Complications
Therapeutic ERCP is generally safe but technically complex and carries some risks. Common complications include:
- Pancreatitis (inflammation of the pancreas), occurring in up to 5–10% of patients
- Bleeding, especially following sphincterotomy
- Infection (cholangitis), if ducts are incompletely drained
- Perforation, which is rare but possible with any endoscopic procedure
These risks are minimized when the procedure is performed by an experienced gastroenterologist in a well-equipped facility.
Recovery and Aftercare
Most patients recover quickly following therapeutic ERCP, though some may experience mild bloating, sore throat, or nausea due to sedation.
Post-procedure recommendations include:
- Resting for the remainder of the day
- Resuming a light diet unless otherwise instructed
- Monitoring for warning signs such as severe abdominal pain, persistent vomiting, fever, or black stools—seek immediate medical attention if these occur
- Attending follow-up visits to ensure bile ducts remain open and symptoms resolve
Why Timely ERCP Matters
Delaying treatment for biliary obstruction may lead to severe consequences, such as:
- Cholangitis—a potentially life-threatening infection that requires urgent drainage
- Liver damage—prolonged obstruction can cause biliary cirrhosis
- Sepsis—a systemic infection spreading through the bloodstream
Thus, therapeutic ERCP is often a lifesaving intervention rather than a mere convenience.
The Role of a Gastroenterologist
ERCP requires specialized training and equipment, making it unavailable in all hospitals or clinics. Gastroenterologists with expertise in therapeutic endoscopy are best suited to perform the procedure safely and effectively.
Patients experiencing jaundice, severe abdominal pain, or unexplained changes in urine or stool color should seek prompt evaluation. Early referral to a gastroenterologist allows for faster diagnosis, treatment, and recovery.
Final Thoughts
Therapeutic ERCP is a cornerstone of modern gastroenterology for managing biliary obstruction caused by gallstones, strictures, and cancer. By combining diagnosis and treatment in one session, it provides rapid relief, reduces complications, and improves patient outcomes.
If you or a loved one have symptoms suggestive of bile duct obstruction—such as jaundice, dark urine, pale stools, or unexplained abdominal pain—do not delay seeking medical attention. An experienced gastroenterologist can determine if therapeutic ERCP is appropriate and guide you safely through the process.
About Dr. Deetlefs
Dr. Deetlefs is a highly respected gastroenterologist based in Cape Town, recognized for his expertise in diagnosing and treating a wide range of gastrointestinal (GI) conditions. With years of clinical experience and a patient-centered approach, he is dedicated to providing advanced, evidence-based care for issues such as acid reflux, inflammatory bowel disease, liver and biliary disorders, and colorectal cancer screening.
Combining state-of-the-art technology with compassionate care, Dr. Deetlefs ensures accurate diagnoses and effective treatment plans tailored to each patient’s needs. For those experiencing persistent digestive symptoms or in need of a routine check-up, contacting Dr. Deetlefs is a proactive step toward optimal digestive health.
He has earned a reputation as a trusted health expert, providing consultative, diagnostic, and therapeutic endoscopic services to patients in Cape Town and beyond. Dr. Deetlefs can be contacted to confirm the estimated breakdown should you be interested in having the procedure done.
DISCLAIMER: PLEASE READ CAREFULLY
The information on this website is to provide general guidance. In no way does any of the information provided reflect definitive medical advice and self-diagnoses should not be made based on information obtained online. It is important to consult a Gastroenterologist or medical doctor regarding ANY and ALL symptoms or signs including, but not limited to: abdominal pain, haemorrhoids or anal / rectal bleeding as it may a sign of a serious illness or condition. A thorough consultation and examination should ALWAYS be performed for an accurate diagnosis and treatment plan. Be sure to call a physician or call our office today and schedule a consultation.
GIDoc Cape Town
Patient-focused GI treatments and procedures in Cape Town.
Monday-Friday 8AM-4PM.
Connect with Us

© Dr. Eduan Deetlefs, Registered Gastroenterologist, GI Doc Cape Town
Our website information is not intended or implied to be a substitute for professional medical advice, diagnosis or treatment. Please consult a doctor about your specific condition. Only a trained physician can determine an accurate diagnosis and proper treatment.