What is EMR Polypectomy?
You may have heard of the word “polyp” before.
Polyps are abnormal tissue growths that most commonly develop in the colon. They look like small bumps and may even resemble mushroom stalks.
While most polyps are benign (non-cancerous), because it’s an abnormal tissue growth, there’s a high chance it can become cancerous and cause you tons of problems later on.
That’s why polyps need to be examined and removed as soon as possible.
That’s what the EMR polypectomy is for.
EMR Polypectomy
Endoscopic Mucosal Resection, or EMR, is a procedure that involves the removal of polyps or tumors in the digestive tract which may be precancerous or at early stage cancer.
The instrument used in EMR polypectomy is an endoscope – a flexible narrow tube with a light and a video camera at the end that allows the gastroenterologist to see the inside of your body with elaborate details.
The endoscope is passed down to the patient’s throat to reach the site of the polyp either in the patient’s esophagus, stomach, or duodenum (the upper part of the small intestine).
The endoscope may also be guided up through the anus if the site of abnormality is found in the colon.
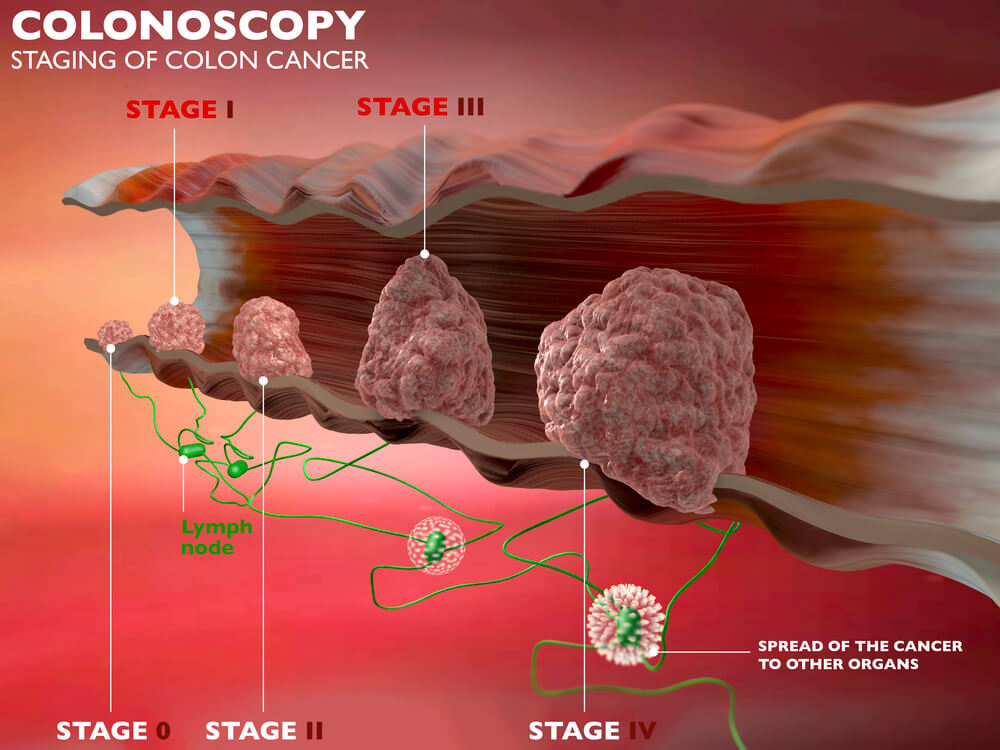
EMR is a curative procedure, but it may also be used for in-depth diagnostic and staging purposes as EMR is also useful in biopsy tissue sampling.
EMR also helps in determining whether cancer cells have already invaded tissues beneath the digestive tract lining.
EMR is also used to treat Barrett esophagus – a condition in which the cells that make up your esophagus begin to look like the cells that make up your intestines as cells were constantly exposed to acid due to years of gastroesophageal reflux (GERD).

What is the Difference between EMR and ESD?
EMR is most effective for tumors that have not yet reached deeper layers of the gastrointestinal wall and are no larger than two (2) centimeters.
If the tumor has already reached deeper layers, your gastroenterologist may suggest an endoscopic submucosal dissection or ESD, a procedure used to remove deep tumors from the GI tract.
What Happens During an EMR Polypectomy?
EMR is a minimally invasive procedure that does not involve an incision.
Because of this, patients usually recover faster and experience less pain compared to open or laparoscopic surgery.
As it is usually done as an outpatient procedure, you will be able to go home the same day unless your doctor recommends otherwise.
Patients will be asked to arrive at the endoscopy unit three or more hours before the procedure to register and provide your medical history, including all taken medications.
Before the Procedure
Your doctor should give you written instructions on how to prepare for the EMR.
This usually involves fasting and emptying the colon, which is extremely important for your doctor to clearly see what’s going on inside your body.
You will also need to go on a strict clear liquid diet the day before the procedure.
A liquid laxative or an over-the-counter enema kit might also be prescribed to help empty out the colon.
Once you arrive at the clinic, a nurse will ask you some questions and fill up the necessary paperwork. You will then be asked to change into a gown.
Your pulse and blood pressure will be checked, and a small needle will be inserted into the back of your hand.
Your doctor should also explain to you the procedure, the benefits and risks, and answer any questions that you may have.
You will be asked to sign a consent form to confirm your understanding of what the gastroenterologist has explained and to signify your consent to the procedure.

During the Procedure
You will be asked to remove false teeth or glasses before lying down on a trolley on your left or right side, whichever is comfortable for you.
Your doctor will give you sedation to make you feel relaxed and drowsy.
Pain relief will also be administered.
The sedation is not a general anaesthetic. You will still be able to hear the nurses/doctor talking to you. However, the effect of sedation may cause you to not remember the procedure afterward.
You will also be given oxygen to aid in breathing.
The endoscope will be gently inserted through the mouth/anus, wherever the location of the tumor, and images of your GI tract will be observed by the doctor on the screen.
Sometimes, applying a suction to the top of the tumor is necessary to further lift the tumor up away from the other tissue.
This prevents creating further damage to the surrounding tissues during the procedure.
Your doctor will then insert a thin wire rope through the endoscope to cut the tumor at its base and seal the cut at the same time.
The tumor will then be retrieved through suction and pulling through a specialized retrieval tool that will be passed through the endoscope.
A laboratory examination will confirm if the tumor has been completely removed from the GI tract.

After the Procedure
After the procedure, you will be transferred and monitored in a recovery room while the sedative wears off.
Occasionally, the sedative lowers the blood pressure and may also cause breathing problems. This makes it important to closely monitor your pulse and blood pressure before being cleared to go home.
Before you leave the facility, your gastroenterologist will discuss after-care and the next steps you need to take.
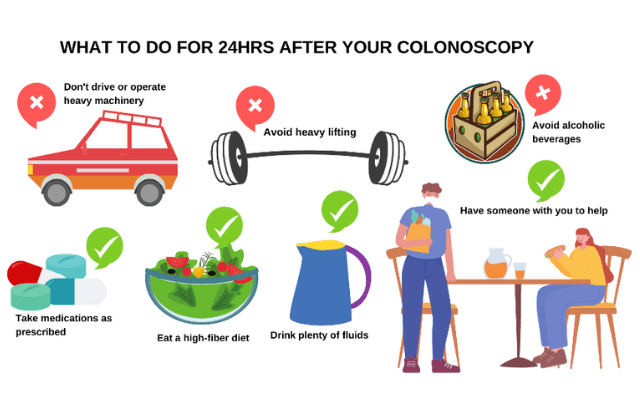
You shouldn’t drive (vehicle insurance will become invalid), operate any machinery, drink alcohol, or sign any legally binding documents within 24 hours after the procedure.
At home, you may drink or eat as normal, but try to eat a high-fiber diet.
Some of the after-effects of EMR include slight bloating and bleeding, sore throat, nausea, and vomiting. These are normal and should subside within 24 hours. If not, call your doctor immediately.
What are the Risks of EMR?
EMR is proven to be a safe and effective technique in the management of GI lesions when performed by an experienced gastroenterologist or endoscopist, given that it is applied only on an appropriate lesion.
Bleeding is the most common complication during EMR that can be detected and corrected even during the procedure.
There’s an extremely slight chance (1 in every 1500 people) for you to suffer a perforation or significant bleeding that requires an operation and/or blood transfusion.
There is also a slight risk of narrowing of the esophagus which may lead to difficulty in swallowing and may require further treatment.
There may also be a slight risk of puncture on the site where the lesion has been removed.
If you develop fever, chills, vomiting, black stool, bright red blood in the stool, chest or abdominal pain, shortness of breath, and/or fainting after undergoing EMR, you must seek medical attention immediately.
With that said, the chances for these complications to happen are very slim. When properly done, the benefits of EMR far outweigh the risks.

Follow-Up Appointment
You will likely have a follow-up appointment with your doctor to discuss the results and findings of the EMR.
It is important to ask your doctor if they were able to remove all the abnormal tissues and if there were any cancerous among those tissues.
Three to twelve (3-12) months after the procedure, a follow-up exam may be performed to make sure that all abnormal lesions have been completely removed from the GI tract.
EMR polypectomy is a safe procedure that has saved millions of lives.
In the care of a good gastroenterologist, the procedure should go smoothly without any hitch.
If you need a trusted gastroenterologist to perform your EMR polypectomy in Cape Town, give Dr. Deetleefs a call today.
DISCLAIMER: PLEASE READ CAREFULLY
The information on this website is to provide general guidance. In no way does any of the information provided reflect definitive medical advice and self-diagnoses should not be made based on information obtained online. It is important to consult a Gastroenterologist or medical doctor regarding ANY and ALL symptoms or signs including, but not limited to: abdominal pain, haemorrhoids or anal / rectal bleeding as it may a sign of a serious illness or condition. A thorough consultation and examination should ALWAYS be performed for an accurate diagnosis and treatment plan. Be sure to call a physician or call our office today and schedule a consultation.
GIDoc Cape Town
Patient-focused GI treatments and procedures in Cape Town.
Monday-Friday 8AM-4PM.
Connect with Us

© Dr. Eduan Deetlefs, Registered Gastroenterologist, GI Doc Cape Town
Our website information is not intended or implied to be a substitute for professional medical advice, diagnosis or treatment. Please consult a doctor about your specific condition. Only a trained physician can determine an accurate diagnosis and proper treatment.












 Irritable Bowel Syndrome
Irritable Bowel Syndrome


